
I am sure you saw the actual video tape, though we have known this was coming. President Obama has announced a plan to deploy up to 3,000 US Military personnel to combat the outbreak of the deadly Ebola disease in West Africa. Those forces will require a unique fusion of medical and force protection intelligence to accomplish their mission.
As President Obama announced in mid-September of 2014, combating the outbreak:
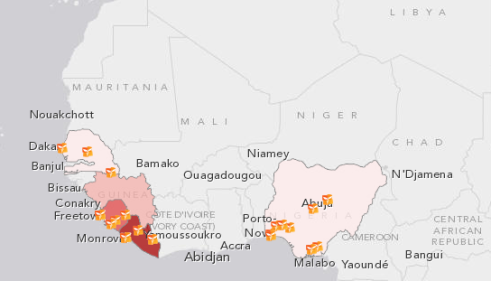
“…is a top national security priority for the United States. In order to contain and combat it, we are partnering with the United Nations and other international partners to help the Governments of Guinea, Liberia, Sierra Leone, Nigeria, and Senegal respond just as we fortify our defenses at home. Every outbreak of Ebola over the past 40 years has been contained, and we are confident that this one can – and will be – as well.”
The announced strategy is predicated on four key goals:
· Control of the epidemic at its source in West Africa;
· Mitigating second-order impacts, including blunting the economic, social, and political tolls in the region;
· Engaging and coordinating with a broader global audience; and
· Fortifying global health security infrastructure in the region and beyond.
In order to accomplish these missions, plus the unstated but vital force protection issue and Indications and Warnings of attempts to “weaponize” the disease by deliberate attempts to export the contagion, a new and comprehensive communications architecture and analytic and medical intelligence support is necessary for mission accomplishment. In addition to command and control, logistics expertise, training, and engineering support, all-source intelligence support is required to support the mission.
One focus will of course be the Joint Force Command, a component of US Africa Command, headquartered in Monrovia, Liberia. This central node will provide on-site regional command and control support to US military activities and facilitate coordination with US government and international relief efforts, which will involve an estimated 3000 US forces. Effective connectivity with the national, regional and international elements in effective response is necessary immediately.
The Threat Vector

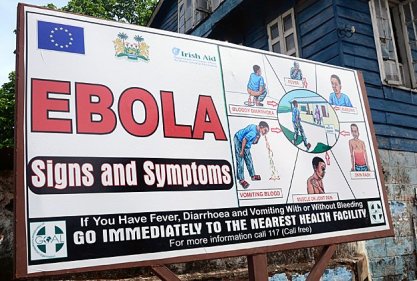
Ebola is an infectious and often fatal disease that results in fever and severe internal bleeding. There are no medications effective in curing the virus, but supportive hospital care can significantly increase survival. Ebola is highly contagious through infected bodily fluids like sweat, blood, and saliva and remains infectious even after the victim has died.
It is a daunting dramatic threat to a region with underdeveloped health resources, crushing poverty and a legacy of decades of armed conflict.
In the US, Response to public health emergencies is provided by a sector-based approach shared between the Department of Health and Human Services and its components (Center for Disease Control (CDC) National Institutes of Health, et al), State, local, tribal, and territorial levels of government.
This structure generally corresponds to the scales on which emergencies generally occur. On the one hand, the complex and dispersed nature of the sector makes it difficult to disable the entire nationwide system. On the other hand, this presents challenges in coordinating emergency responses across disciplines, regions, and levels of government- a fact that is exacerbated by the fact that this is a military response, out of the Continental US, and conducted in the face of multiple al Qaida affiliates in the region, the prime one being Boko Haram, but with other regional terror organizations also playing a role in the force protection problem.
The prospect of American Boots on the Ground this presents a multi-faceted threat environment in which effective warning must fuse together two related but quite different disciplines: all-source intelligence threat Indications and Warning, and classic methods of epidemiology.
All-Source Analysis
Intelligence products and/or organizations and activities that incorporate all sources of information, most frequently including human resources intelligence, imagery intelligence, measurement and signature intelligence, signals intelligence, geo-spatial information and open-source data in the production of finished intelligence. Additionally, “pattern of life” and other socio-cultural aspects of the all-source picture must be integrated in any comprehensive intelligence solution. Experience in supporting tactical units in Afghanistan clearly demonstrates that augmentation to forces in the field is the most effective means of improving mission accomplishment. Collection management support to the analytic process is absolutely essential in the development of spiral response to evolving situations.
Epidemiology
Epidemiology is the study of patterns, causality and effect of disease on public health in defined populations, which in the case of Ebola crosses national and ethnic boundaries. It is the cornerstone of public health response to epidemics, and informs policy by identifying risk factors and means of prophylaxis to them. In the case of the Ebola outbreak, sentinel data collection is one of a number of assessment tools to identify, catalogue and sequester threat vectors for infection. Using statistical analysis and direct observation, a variety of clinical approaches to define best course of treatment and likely drug therapy will result in managing the crisis, which is spreading in a region battered by civil strife and terrorist insurgencies against post-colonial nation states. Major areas of epidemiological study include disease etiology, transmission mechanisms, outbreak tracking, investigation and clinical investigation to better understand how Ebola processes and the means to break the cycle of infection and the proximate and distal causes to break the chain.
The two disciplines- one medical and the other intelligence- employ similar and parallel methodologies. Our solution brings them together in close coordination.
Why an Integrated Response is Necessary
The Great Pandemic, 1918
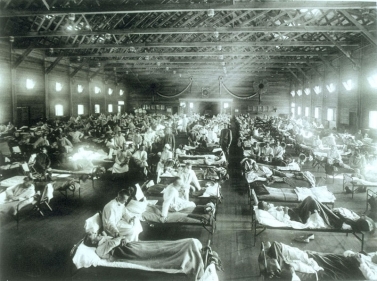
(Army hospital at the height of the influenza pandemic. Photo US Army)
The US Government has confronted global medical emergencies before. Perhaps the most deadly of them- and a cautionary one in the context of the emerging Ebola Crisis- was the great influenza pandemic of 1918-1919. “Spanish Flu,” or “Grippe” killed more people than the total lost in World War I, at somewhere between 20 and 40 million people. It has been cited as the most devastating epidemic in recorded world history.
In America, An estimated 675,000 perished from a population of only slightly over 103 million. Of the U.S. soldiers who died in Europe, an estimated 43,000 servicemen died of the Flu.
While the pandemic passed, it remains the nightmare public health scenario: easily communicated, rapidly spread and highly lethal.
A Proposed Response

To summarize, AFRICOM has been directed to deploy a JTF headquarters, build and operate a logistics base (the ISB), build a hospital and other treatment facilities, conduct training for host nation personnel, and provide air transportation. None of these capabilities are “unique” to the US military, though arguably only the US has the integrated capability to conduct global operations of this scale.
Due to the nature of this threat, however, the capabilities and resources of the whole-of-government response are required, which could range as far afield as the Veteran’s Administration, which maintains a challenged (but significant) infrastructure.
Applying this whole-of-government approach, we have been engaged in various levels of response since March, when the first cases were reported in West Africa. Currently more than 100 specialists from multiple US departments and agencies, including HHS, CDC, US Agency for International Development (USAID), and DoD are engaged, but their efforts require robust and secure communications due to the force protection and terror components present in the region.
Accordingly, the various components of the United Nations must be connected to any comprehensive solution. These include the World Health Organization, the governments of the affected countries, and other partners, including the United Kingdom, France, Germany, Norway, the Africa Union, and the European Union.
The SARS Response as Template
The response to the SARS outbreak was the formalization of responsibilities under the new Critical Infrastructure Protection Plan drafted by the newly consolidated Department of Homeland Security. The Office of Public Health Emergency Preparedness (OPHEP) was created on the staff of the HHS Secretary as a prudent measure in the wake of 9/11m and the real fear that weapons of mass destruction would be used against the Homeland.
Instead, real events demonstrated the utility of a coordinating organization to confront natural and human-induced health disasters.
SARS
Severe acute respiratory syndrome (SARS) is a serious form of pneumonia. It is caused by a virus first identified in 2003. Infection with the SARS virus causes acute respiratory distress that can lead swiftly to collapse and death. A cross-species infection first identified in Hong Kong, patients traveled to Vietnam and Canada before the virulence of the infection was recognized. Between November 2002 and July 2003, 8,273 cases and 775 deaths were reported in 37 countries with a fatality rate of 9.6% for those infected.
In r established an active watch in a dedicated space in the HQ that was linked by video and communications (with the Joint Worldwide Intelligence Communications System (JWICS) as necessary) to CDC in Atlanta and with regular communications with the World Health Organization.
The DoD Focal Point
The Ebola Outbreak is taking place in a region with active insurgencies and an emerging terrorist threat, which requires the integration of all-source intelligence analysis from the IC for indications and warning and force protection. The organization within the Department of Defense charged with intelligence assessments of epidemiological threats is the National Center for Medical Intelligence. Located at Fort Detrick, MD, the NCMI is a joint-service component of the Defense Intelligence Agency. With origins in the Army’s campaign against Yellow Fever, and later the influenza epidemic, NCMI is organized into a support division and two substantive divisions—the Epidemiology and Environmental Health Division and the Medical Capabilities Division.
The Environmental Health Division has direct application to the Ebola outbreak through its mission to Identify and assess environmental risks that can degrade force health or effectiveness including chemical and microbial contamination of the environment, toxic industrial, chemical and radiation accidents, and environmental terrorism/warfare.
Additionally, MCMI is the ideal entity to identify, assess, and report on infectious disease risks to the force itself that can degrade mission effectiveness of deployed forces and/or cause long-term health implications.
Summary
The situation is well past the containment phase in Liberia, where the major US military footprint will be located. The key to containment is the application of epidemiological methodology to an all-source analytic capability targeted at the force protection threat as well as the threat to the homeland.
This requires direct connectivity with the Public Health Emergency system, drawing on the basic sector alignment established in the health annex to the DHS National Infrastructure Protection Plan. In that context, we know how to provide emergency medical care at the scene of the contagion, during infectious disease outbreak, and during patient transport and delivery to a hospital or other treatment facilities.

The trick is linking what we do here to the military capability to establish treatment centers where they are needed and add in the military force protection capabilities to the all-source analytic process. Boko Haram is active in the area, and quite capable of exploiting the presence of US forces for terror operations.
Not to mention that they are quite capable of using the Ebola as a weapon of terror as well.
So, this is a multifaceted challenge that we are actually well positioned to address through linked Intelligence Operations systems appended to the National Medical Intelligence Center at Fort Detrick, the Pentagon and the Joint Staff Crisis Action Group (AG), the Department of Health and Human Services, CDC in Atlanta and collateral links to the WHO in Geneva, the Department of Homeland Security and Customs and Border Protection, national governments in the areas of contagion, along with connectivity to host nations, AFRICOM and JIOC Dets with deployed forces. It is those detachments, located physically in the areas of contagion, which will require real-time force protection
They would then be able to provide threat assessments (health and force protection) as well as monitor the three “T’s” of the outbreak: triage, treatment, and transport of all Ebola infections to central treatment points.
We also propose that this network will be responsible for both preparing US and host nation staff, patients, facilities, and environment; providing response teams with the situational awareness on comprehensive medical care and mental health support to patients and their families, comprehensive force protection and indications and warning support to deployed forces. .
We know how to do this- the key is to adapt what we do to a mission that is analogous (epidemiology) with all-source intelligence needed to provide effective response, situational awareness across West Africa, and the potential for global outbreak.
There is also a darker threat inherent in the outbreak of any virulent disease. There are adversaries who could weaponize the Ebola epidemic by deliberately exposing volunteers who hold valid EU/US passports and dispatch them to infect as many people in their home countries as possible.
Directly harnessing our experience with Pattern of Life/Attack the Networks expertise gained in Iraq and Afghanistan will bolster our ability to interdict such plots as they are in progress.
With potential deaths in the millions and the Ebola outbreak uncontained, it is beyond time for a coordinated effort within the US Government between the IC, DoD, the Inter-agency Public Health sector (which includes the resources of the VA), DoJ and DHS components. All can share information via the Joint Worldwide Intelligence Communications System (JWICS), while recognizing that connectivity is not as robust in the public health sector and requires investment.
Parallel fire walled connectivity is required outside the US Government, including Non-governmental entities, host nation defense and health entities, and donor partners. Thankfully, extensive coalition operations over the last decade have eased the intrinsic conflict of interoperability across jurisdictional lines.
The architecture will require careful but rapid development, and the provision of analysts familiar with the parallel All Source and Epidemiology communities.
Haste is required. The threat is real and it is imminent.
Copyright 2014 Vic Socotra
www.vicsocotra.com
Twitter: @ jayare303